Skip to content
Skip to content

Are you struggling with Hard Flaccid Syndrome (HFS) and looking for an experienced hard flaccid doctor in New York? You’re not alone. HFS affects many men and can cause persistent discomfort, semi-erect or flaccid penis, and pelvic pain. Unfortunately, it’s often misdiagnosed or misunderstood. The vast majority of patients are left frustrated because many medical professionals are unfamiliar with HFS as a clinical diagnosis. HFS is a relatively new clinical diagnosis, which contributes to the lack of proper diagnosis and effective treatment.
Dr. Adam Gvili, a specialist in pelvic floor therapy, offers personalized HFS treatment in NYC at his specialized clinic, providing expert care to help men regain sexual function, reduce pain, and improve quality of life.
What is Hard Flaccid Syndrome (HFS)?
Hard Flaccid Syndrome is a condition where the penis remains in a semi-rigid or “half-hard” state, even at rest. This is a clinical manifestation involving both the erect and flaccid penis, and is due to excessive tightening of the pelvic floor and penile muscles.
Common symptoms include:
- Semi-erect or flaccid penis at rest
- Pain or discomfort in the penis or pelvic region
- Penile pain
- Painful ejaculation
- Sexual dysfunction or decreased arousal
- Tight pelvic muscles and discomfort around sit bones
- Autonomic symptoms (such as changes in sweating or heart rate)
- Altered sensation along the penis shaft
These clinical manifestations can dampen sexual arousal and make it difficult to achieve a fully hard erection.
Unlike erectile dysfunction, HFS is primarily a muscular and neurological condition, not a vascular or hormonal issue. The prevailing thought was that HFS was only caused by excessive masturbation, but it can also be related to sexual trauma, pelvic floor muscle dysfunction, and athletic injuries. Overactive pelvic muscles can compress nerves and blood vessels, causing pain and sexual difficulties.
To properly identify HFS, a thorough understanding of the nervous system, body alignment, and chronic stress is necessary, as these factors contribute to muscle tension and symptoms. Chronic stress and anxiety can cause the pelvic muscles to contract and tighten, perpetuating the condition.
Understanding Pelvic Pain
Pelvic pain is a frequent and distressing symptom for men with hard flaccid syndrome. This discomfort can manifest in the pelvic floor area, penis, or even radiate to the surrounding tissues, often making daily activities and sexual function challenging. The underlying cause is typically pelvic floor muscle dysfunction, where increased muscle tension restricts blood flow and contributes to ongoing pain and a flaccid or semi-erect penis.
In some cases, pelvic pain is closely linked to erectile dysfunction, as the pelvic floor muscles are essential for achieving and maintaining an erection. When these muscles are tight or overactive, they can disrupt normal function and lead to persistent discomfort. Physical therapy, especially manual therapy and targeted exercises, is highly effective in addressing the root cause of pelvic pain. By focusing on the pelvic floor muscles, therapy can help restore proper blood flow, reduce muscle tension, and provide lasting relief from pain. Addressing pelvic pain early and thoroughly is key to preventing further complications and improving overall quality of life.
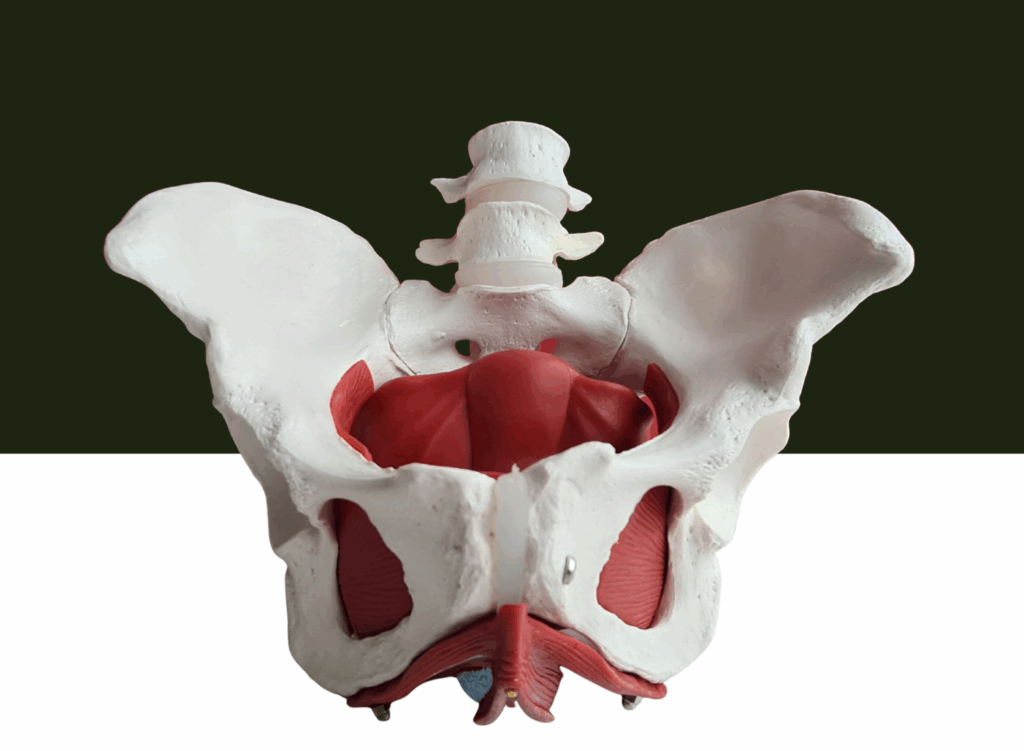
The Role of the Pelvic Floor
The pelvic floor is a complex group of muscles that supports the bladder, bowel, and sexual organs, playing a vital role in men’s health. In hard flaccid syndrome, these pelvic floor muscles can become overactive or tense, leading to reduced blood flow to the penis and a persistent semi erect state. This muscle tension not only affects the ability to achieve a full erection but can also cause a range of symptoms, from discomfort to sexual dysfunction.
Beyond sexual health, the pelvic floor muscles are responsible for controlling urination and bowel movements. Dysfunction in this area can result in issues like urinary incontinence or constipation, further impacting daily life. Treating hard flaccid syndrome requires a comprehensive approach that addresses not just the physical symptoms, but also contributing factors such as anxiety, stress, and sexual trauma. By focusing on the pelvic floor and its role in overall pelvic health, effective treatment can help restore normal function and alleviate the symptoms of hard flaccid.
Causes of Hard Flaccid Syndrome
Many men mistakenly believe HFS is caused only by excessive masturbation, but the condition is more complex. Common contributing factors include:
- Overuse of pelvic muscles or chronic tension
- Athletic injuries or repetitive strain
- Sexual trauma or psychological stress
- Chronic anxiety or stress
- Underlying medical conditions (e.g., UTIs, prostate issues, neurological disorders)
HFS symptoms often follow trauma to the penis or pelvis, such as vigorous sexual activity or intense exercise. Identifying contributing factors is essential for effective hard flaccid treatment, as a thorough evaluation by a specialist can help pinpoint the specific causes and guide targeted therapy.
High-intensity sports or long periods of sitting/standing can further strain pelvic muscles. Understanding these causes is crucial for effective HFS treatment in NYC. Successful treatment depends on identifying the factors perpetuating the dysfunctional reflex loop and using therapies that increase blood flow to the pelvic area.
Diagnosing and Managing Symptoms
Properly diagnosing hard flaccid syndrome is essential, as its symptoms often overlap with other conditions like erectile dysfunction and pelvic floor dysfunction. A thorough evaluation by a knowledgeable medical professional, such as a pelvic floor physical therapist, is crucial to identify the involved musculature and pinpoint contributing factors. This process typically includes a detailed medical history, a physical examination, and sometimes diagnostic tools like ultrasound or digital rectal exams.
Once hard flaccid syndrome is confirmed, treatment focuses on addressing the root cause—often pelvic floor muscle tension, anxiety, or stress. Physical therapy plays a central role, using exercises and manual therapy to improve blood flow, reduce muscle tension, and restore healthy pelvic floor function. In some cases, managing underlying medical issues such as prostate conditions or urinary tract infections is also necessary for lasting relief.
Identifying and addressing contributing factors—such as excessive masturbation, athletic injuries, or sexual trauma—is key to developing an effective treatment plan. By taking a comprehensive approach and working closely with experienced medical professionals, most men can achieve significant improvement and regain confidence in their sexual and pelvic health.
How Physiotherapy Helps Treat HFS
Pelvic floor physical therapy is one of the most effective ways to treat Hard Flaccid Syndrome, which is now recognized as a clinical diagnosis requiring a thorough evaluation by a Men’s Health Physical Therapist. Dr. Adam Gvili specializes in evidence-based HFS treatment tailored to each patient’s needs.

His approach includes:
- Pelvic floor muscle retraining to reduce involuntary muscle tension and restore normal pelvic coordination
- Manual therapy including myofascial release, trigger point therapy, and joint mobilizations to address mechanical restrictions
- Dry needling targeting deep myofascial trigger points and assisting in neuromuscular reset
- Focused Shockwave Therapy designed to improve blood flow to the pelvic area and stimulate muscle relaxation
- Relaxation and stretching exercises to improve blood flow and reduce discomfort
Patients are encouraged to practice regular pelvic floor relaxation and stretching exercises between appointments. Managing emotional distress, such as anxiety and depression, is also important for individuals suffering from HFS. When consulting a doctor about HFS, patients should detail their symptoms, medical history, and potential triggers, and communicate clearly for an accurate evaluation. Persistent symptoms such as a consistently semi-rigid penis, pelvic pain, and urinary changes warrant consultation with a healthcare professional.
Patients are guided with at-home exercises to maintain progress and support long-term improvement.
A Holistic Approach to HFS Treatment
Dr. Gvili takes a comprehensive approach to Hard Flaccid Syndrome, addressing both physical and emotional aspects of the condition. Stress, anxiety, and psychological factors can worsen HFS symptoms. HFS can create a vicious cycle with stress, affecting both the body and psychological well-being, which complicates both the psychological and physical presentation of the condition.
By combining physiotherapy with counseling and stress management, Dr. Gvili helps patients:
- Reduce pelvic tension
- Improve sexual function
- Improve sexual activity and support holistic body relaxation and alignment
- Increase confidence and overall quality of life
Why Choose Pelvis NYC for HFS Treatment?

When searching for a hard flaccid doctor in New York, Pelvis NYC offers:
- Specialized HFS treatment in NYC
- Patient-centered care tailored to your unique needs
- Expertise in pelvic floor physiotherapy
- Support for both physical and emotional recovery
Take the first step toward lasting relief. Schedule a FREE 15-minute teleconsultation with Dr. Adam Gvili, a hard flaccid doctor, and start your journey to better pelvic health today.